
Blast overpressure (BOP) is defined as the sudden onset of a pressure wave, above normal atmospheric pressure, which occurs from blast (e.g., explosions and weapons firing events).
In a memorandum dated 8 August, 2024, the Deputy Secretary of Defense has updated requirements for managing brain health risks from often overlooked sources of overpressure. In addition to BOP from exposure to Improvised Explosive Devices (IED) they have taken a look over the past few years at overpressure caused by our weapons during training and operations.
This new directive, which goes into effect immediately, expands the June 8, 2022 memorandum, “Department of Defense Warfighter Brain Health Initiative – Strategy and Action Plan” and rescinds Assistant Secretary of Defense for Readiness Memorandum, “Interim Guidance for Managing Brain Health Risk from Blast Overpressure,” November 4, 2022.
It further establishes DoD requirements and direction for the management of health risks to DoD personnel from exposures to BOP. However, there’s no intent to preclude or unreasonably restrict commanders from conducting mission-essential weapons training. Rather, this policy establishes requirements for practical risk management actions to mitigate and track BOP exposures across the DoD.
The memorandum states, “Experiences by DoD personnel in training and operational environments demonstrate possible adverse effects on brain health and cognitive performance ( e.g., headache, decreased reaction time, attention difficulty, memory loss) resulting from acute (e.g., single or short-term) and chronic (e.g., repetitive or continuous) exposure to BOP. Brain health effects from BOP exposures are not yet fully understood, but adverse health and cognitive performance impacts have been reported from acute exposures to BOP above 4 pounds per square inch (psi).”
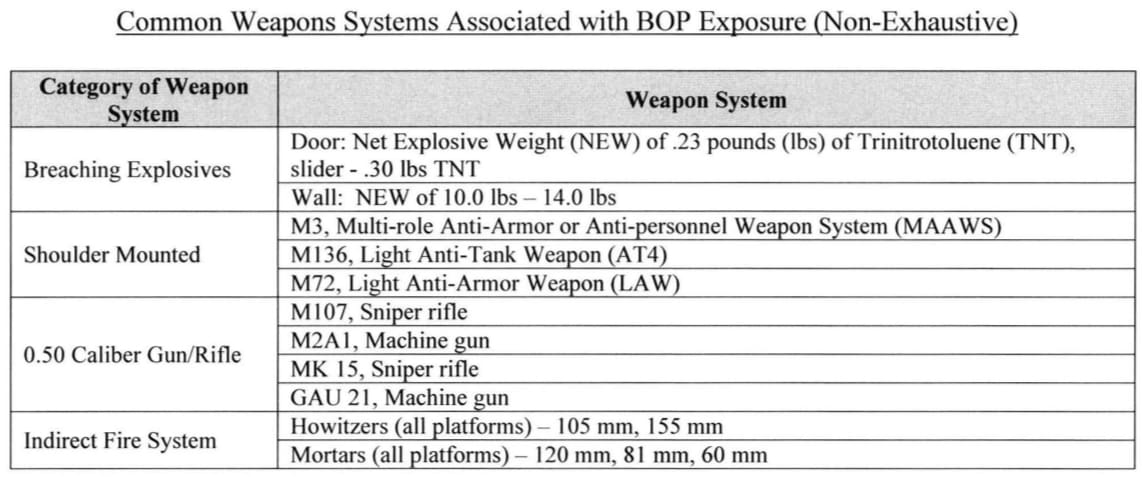
Consequently, DoD is instituting an interim BOP exposure safety guideline of 4 psi will be used as a threshold to require initiation of appropriate risk management actions until further research is complete. Weapons systems known to produce BOP exposures exceeding 4 psi include breaching charges, shoulder fired weapons, 0.50 caliber rifles/guns, and indirect fires.
In addition to increased screening for the effects, units will implement several measures to mitigate the risk of brain injury, including at a minimum:
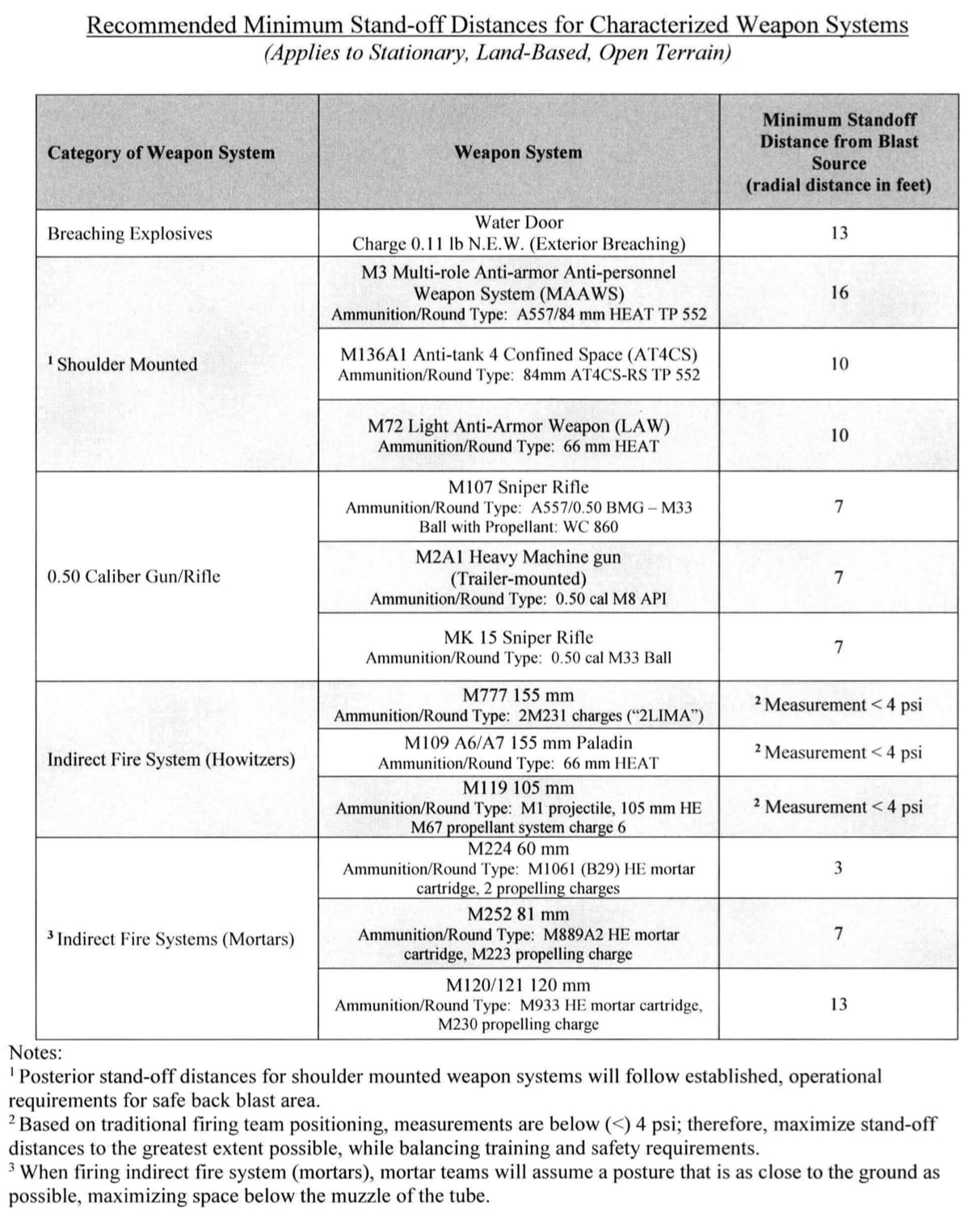
– Stand-off distances for personnel involved in training (e.g., instructors, range safety officers) The “DoD Blast Overpressure Reference and Information Guide” may be used as a resource to support implementation efforts, located at Health.mil/BrainHealthRisk.
– Stand-off distances for non-training audiences that maximize distance from the weapons system to the greatest extent possible.
– Personal protective equipment for firers, trainers, and other personnel at an increased risk of BOP exposure.
– Minimize the number of personnel in the vicinity of BOP generating events (i.e., personnel who are not directly involved in the training or executing tasks associated with the training event) to minimize unnecessary exposure.
The memorandum also contains a rather long list of military specialties which have an increased list of last overpressure exposure but it’s definitely not comprehensive. For example, it lists Army MOS 11A and 11B but ignores 11C and 11Z. Likewise, 19D is listed but not 19A, 19B, 19C, 19K or 19Z. Oddly, on the Air Force portion of the list, someone thought to include the Special Warfare officer codes, but not the enlisted ones.
Download your copy here.
The list of increased overpressure exposure has the same problem that the noise exposure lists have in that it doesn’t take into account any support MOS’s.
Artillery typically has 68W (medics), commo, etc. attached that are on the gun line but given the variability in those jobs (line medic vs hospital, etc.) none of them ever make these lists.
The issue is then compounded when the VA over-relies on these lists later and won’t take in other context. I literally got told by an examiner “as a medic, you’re on the low noise exposure list so you can’t possibly have tinnitus” despite the fact that I spent 6yrs on the gun line as a medic.
I’m currently in the middle of being evaluated by the VA for memory problems and getting shut down when mentioning the various studies that have already been done on low level blast exposure and chronic concussion.