
The U.S. Army Medical Materiel Development Activity has teamed with one of its commercial partners in the development of a novel medical device that may prove to be a “game-changer” in the frontline treatment of wounded Warfighters. Created by TDA Research, Inc., and funded through the Defense Health Agency’s Small Business Innovation Research program, the Lactated Ringer’s Solution Generator is a lightweight, portable unit that can produce sterile LR solution in austere locations from locally available freshwater sources. The device utilizes proprietary technology to produce one liter-size intravenous bags from a concentrated LR salt solution.
Composed of sodium, chloride, potassium, calcium and lactate, LR solution is used primarily to treat dehydration, deliver medication and restore fluid balance following bodily injury. It is also used to treat moderate hemorrhagic shock, as it has been shown to increase initial survival rates among patients and decrease the chances of organ damage.
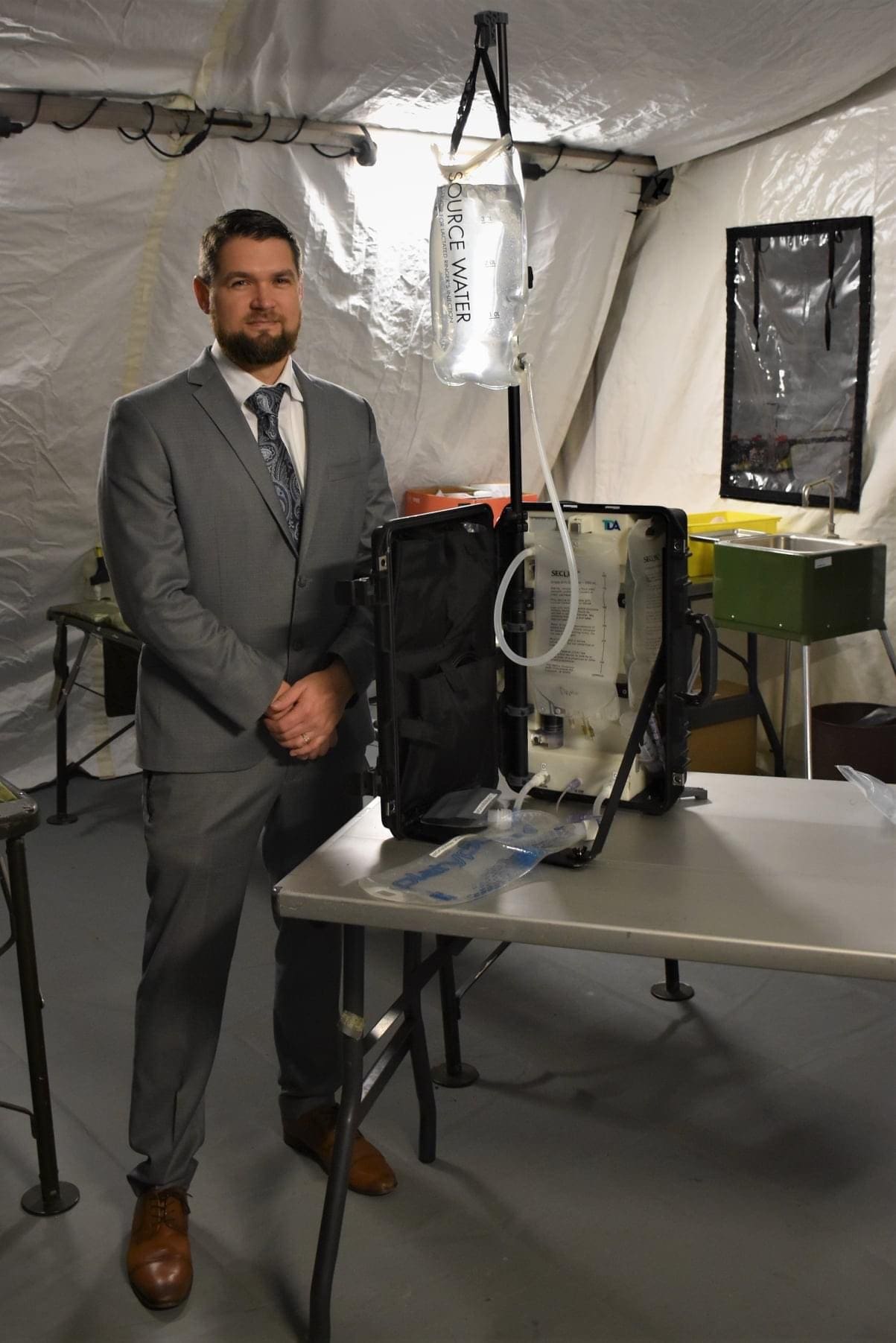
Austin Langdon serves as assistant product manager for the LR Solution Generator program within USAMMDA’s Warfighter Deployed Medical Systems Project Management Office. He believes the device will help to save lives on the battlefield, and recently he demonstrated the unit for Army Brig. Gen. Michael J. Talley, Commanding General of the U.S. Army Medical Research and Development Command and Fort Detrick.
“Without question, this small device will dramatically reduce the Army’s logistical footprint of having to ship and store lactated Ringer’s solution, which is the fluid of choice for resuscitation if blood is not available on the battlefield,” said Langdon. “This unit can make LR solution from practically any water source, including ditch water.”
“I truly believe in this device and its application for military use in the near future, although it will probably find its way into civilian medicine as well,” he continued. “For the Army, the LR Solution Generator will increase our life-saving capabilities by helping to reduce our logistical supply chain demands — our ability to make LR solution in the field will also help ensure we’re able to use these critical bags before they expire.”
As a former Army flight medic, Langdon praised the unique qualities of the device, highlighting its size, weight and portability. The unit weighs less than 11 pounds and is stored in a hard-shell case that is approximately 10 inches wide by 18 inches long, and only 6 inches deep. The purification device runs on a rechargeable lithium-ion cell that can produce more than 30 bags of LR solution per single charge.
“Army leadership is continually seeking ways to reduce the logistical strain of getting much-needed resources to the frontline and far forward in Multi-Domain Operations,” said Langdon. “Products such as the LR Solution Generator are far-forward-leaning solutions that can help us think outside of our normal parameters of operation. This device, and others like it, will bring forth new innovation that will change our standard of operation and secure our valuable resources.”
By Jeffrey Soares, USAMMDA public affairs
Ton of questions, but mostly the fine points- bags themselves and admin sets, outer bags for storage?, prefilled cartridge ?…… Should be a Godsend for burns. On weight savings alone- 86% for one battery charge>almost 100% with solar . While it’s technically possible to make and bottle LR before this- it’s a long way from practical or safe. Simply amazing, soda fountain for LR!
Pointless. This was seen and discussed by the current flight medic community. We have gotten away from lactated ringers and normal saline. Saline is pretty much only used to administer drugs and LR for burns. The benefits over carrying a bit of LR around is nullified by having a new product that requires training, additional resources, and a fat check to use. Creating solutions for problems that don’t exist.
That’s not the end all of the argument, you guys need to get off Fisher’s junk and realize not everything is hemorrhagic. 6 months clinic with occasional bad shit , not “bad shit’s all I do!” Trauma Monkey stuff. WBB and FWB is freaking awesome but it applies to like 2-3% of cases at most.
We have already transitioned to near peer and delayed medical practices. We understand trauma is now rare and not the main effort.
We look at this new gee-whiz product and give it accolades when we have tons of readily available at easily transported LR already. While we dump money into a solution that isn’t needed, units throughout the Army are struggling to just get regular supplies to train with, medics are tasked with additional duties and their medical skills are sidelined, and we don’t even have good management of the current medical electronics.
But yeah, let’s get another thing to add to a hand receipt and never use due to its cost and number of components that can be lost. Get real
And for reference, current flight medic, critical care, delayed evacuation care instructor, and all the associated cards and certs for the job.
My concerned is that logistical, this and other maturing tech like it can potentially provide a serious distributed cushioning for any disruption. This certainly isn’t going to save money but it would maintain capability for a while when things get thin. I’ve been around long enough to see several shortages, from Narcan in 2000 to fluids 2° to Puerto Rican factories being without power- the truth is we face this kind of stuff now in relatively unstressed systems. What’s it going to be like when that factory is not just temporarily closed? We’ve got to figure out how to distribute these capabilities. I want to see a bigger one in every hospital pharmacy, medical unit,and ambulance service- something like this as widely distributed as possible. Cost – well ,whatever ,how many does a unit need? Maybe keep your monitors another year and buy a couple….
Curious about the issues with electronics- largely due to propietary batteries and designed obsolescence? An issue across the board- right to repair is a real fight.
Definitely not a “game-changer”, that title goes to the Ranger walking blood bank program. Blood carries oxygen, lactated ringers and normal saline do not. I see some utility for forward deployed surgical teams and hospital units.
If you’re not thinking guerilla hospital, you’re wrong. EABO, Tyranny of Distance, PFC, Expedition Medicine, Under the Umbrella……..
To some of our resident naysayers(in case they’ve forgotten the age-old maxim); there would be no supply/invention for/of this product if there was no demand…
I seem to recall hype over this concept..25?…years ago, then, “poof”. Claims of being able to pour in mud puddle water and get a nice IV solution. Maybe this is the realization of what was being pitched back then.
And guerrilla hospital, or similar delay to definitive care, yes, if we don’t think it through, that is something that is going to smack us one day if we get militarily embarrassed in peer-to-peer.
I want everyone to know that I appreciate that you can have a professional discourse without accusations, name calling or profanity.
Thanks!
Mea culpa, for starting in that direction .
Leave it to the friggin’ medics to keep it civil . . .
I have to disagree…there’s a well-established phrase (“solution looking for a problem”) and a name for the phenomenon (“solutionism” https://en.wiktionary.org/wiki/solutionism).
For many units, I could see the need to bring in fresh water, the bags, the concentrate, etc more work than just hauling in bags of LR. At a Role III, sure, this might not be a bad idea. At a FRSS or CSH…this seems like one more headache.