FORT IRWIN, Calif. — A buzz could be heard as a medical supply drone known as Project Crimson flew overhead to drop off packages of crucial medical field supplies to medics assisting wounded warriors. As the supplies hit the ground, a medic rushed to retrieve the packages, as many of the other medical warriors kept applying field aid to their Soldier counterparts.
The mass casualty scenario, part of Project Convergence 22, brought together medical personnel from the U.S. Army’s 1st Battalion, 7th Cavalry Regiment, and the Australian Army’s 2nd Health Battalion, to experiment with advanced field care technologies, including those enabled by artificial intelligence.
“Project Crimson is a project to take a common unmanned air system and adapt it to support a medical mission,” said Nathan Fisher, Medical Robotics and Autonomous Systems division chief at the U.S. Army’s Telemedicine & Advanced Technology Research Center.
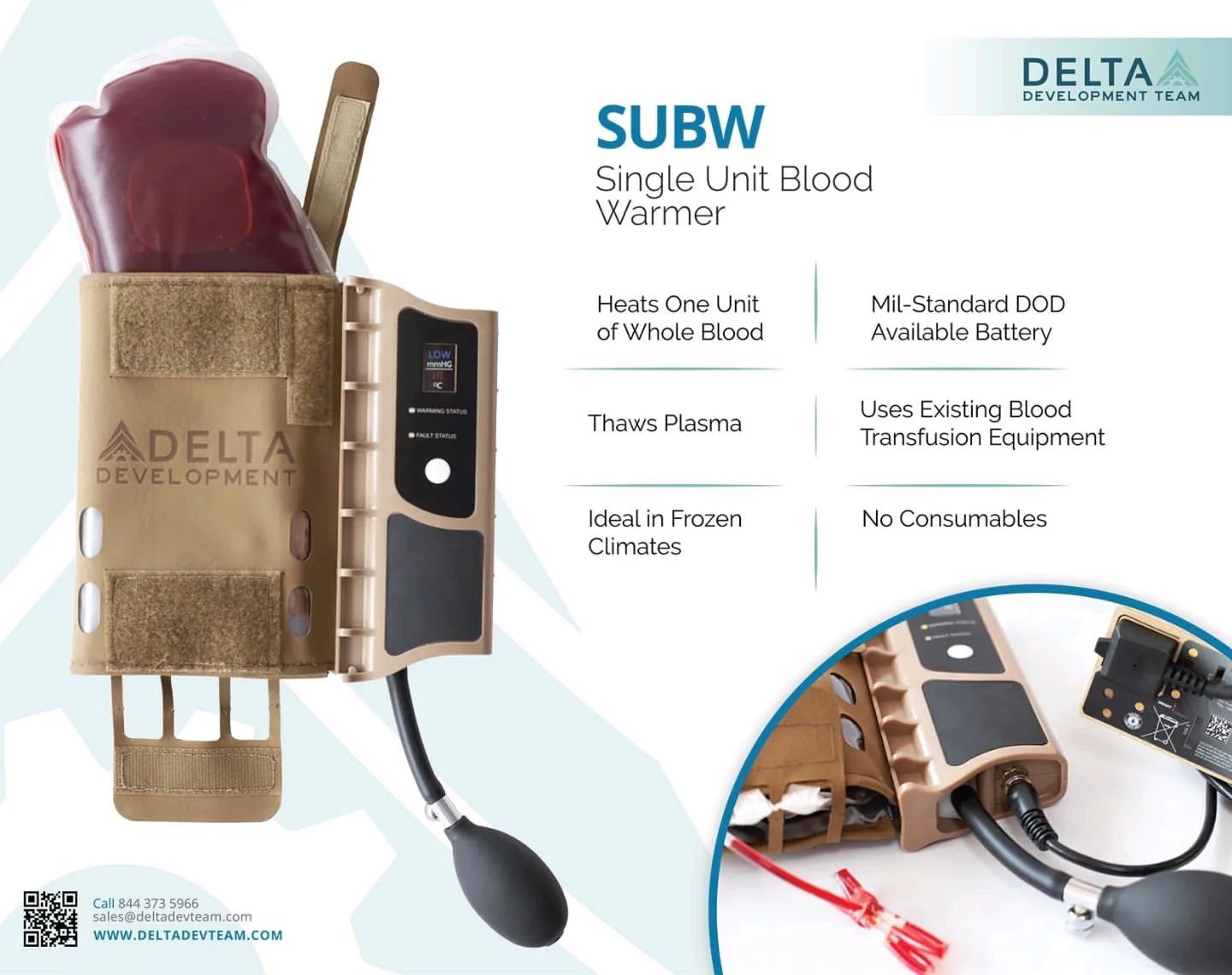
“This drone supports medical field care when casualty evacuation isn’t an option. It can keep whole blood and other crucial items refrigerated in the autonomous portable refrigeration unit and take it to medics in the field with wounded warriors.”
Fisher explained how the drone is a vertical landing and take-off aircraft, therefore doesn’t need a catapult launch or runway to perform a lifesaving mission. This allows military personnel to preserve life in the critical phase of injury and facilitate rapid transport to an Army hospital for further treatment.

While Project Crimson sustained the medical field from the air, military medics used Medical Hands-free Unified Broadcast, or MedHUB, and Battlefield Assisted Trauma Distributed Observation Kit, or BATDOK, systems strapped to their arms and chests to input medical treatments digitally from the ground.
“MedHUB is used to enhance medical situational awareness,” said Philip Featherston, an Air-ground Interoperability and Integration Lab systems engineer. “At the point of injury, we can start hands-free documentation. All we do is place a sensor to the patient that will apply a broadcast to the treatment facility and control center.”
“The facility can see the patient’s status real-time using BATDOK, while the medics on ground can update treatments and medications for the patients as well. This allows the facility to be alerted, rally and prepare to treat the patient once they are transported,” explained Michael Sedillo, an integrated cockpit sensing program airman systems director with the Air Force Research Laboratory.
During the experiment, litters carrying casualties were taken from medical evacuation vehicles, while Army field hospital medics rushed to apply advanced medical care. As casualties were taken into tents, medics with BATDOK and MedHUB systems traded patient information with the previous medical personnel with the near field communication card.
“The ability to have these technologies on hand has enhanced medical field care tremendously,” said Capt. Morgan Plowman, a nurse with the 15th Brigade Support Battalion, 1st Cavalry Division. “To take a tablet or phone to input personnel data has increased the communication down the line and accuracy of field care. So much so that the rate of patient care has increased to the point that caring for a casualty start to finish has sped up drastically.”
The mass casualty experiment also highlighted the potential for allied nations to work together more closely on future battlefields in the area of emergency medical care.
“This is an excellent opportunity to come over here and work with multinational partners,” said Capt. Michael Harley, an Australian Army medical officer, of Project Convergence 22 experimentation. “It is eye-opening to see the initiative between everyone and see the interoperability between the nations.”
“I just came from [advanced individual training], so I didn’t know what to expect coming out here during this event,” said Pfc. Tyler Swanson, a 15th Brigade Support Battalion, 1st Cavalry Division field medic. “When I used this medical technology, it was easy to pick up and learn, even in a fast-paced field environment.”
“I am excited to see what the future of medical technology will look like a decade down the road,” Swanson added.
By SGT Trinity Carter, 14th Public Affairs Detachment